
Knee tendonitis can be a persistent and tricky beast to conquer.
The road to recovery is often paved with ups and downs, false starts and frustrations - sometimes culminating in a less than positive experience for some.
As an industry, we do a great job diagnosing and treating knee tendonitis, but as a Physiotherapist, I often feel we're missing something.
And as I work to better understand the cause and best treatments for knee tendonitis, I've come to learn one surprising thing. Despite a huge lack of focus on this area within the medical industry, it seems the lower back may have a strong role to play in the onset, persistence, and reoccurrence of knee tendonitis.
So in the spirit of sharing I've decided to use the misfortune of one of the Australian Football League's (AFL) best and brightest athletes - Jaeger O'Meara to highlight what I'm finding.
If you're struggling with knee tendonitis hopefully this is the missing piece to your rehab puzzle.
Knee Tendonitis
Knee tendonitis or patellar tendonitis refers to dysfunction of the patellar tendon as it attaches from the bottom of the knee cap to the top of the shin bone.
Originally thought of as an inflammatory condition, most tendon dysfunction has a distinct lack of inflammation. As a result, the correct term for patella tendon dysfunction is actually patella tendinopathy. But to keep things consistent let's just refer to it as tendonitis.
Due to its affinity with jumping and bounding-related activities, knee tendonitis is also known as Jumper's Knee.

Symptoms of Knee Tendonitis
Knee tendonitis is often characterized by pain and tenderness at the front of the knee. Clinically it seems more pain is located closer to the base of the patella than the middle of the Patellar tendon or its insertion into the top of the shin.
Other classic symptoms of knee tendonitis include:
- thickening of the patella tendon
- pain with running, jumping and hopping
- pain that lessens during activity
- post-activity increase in pain
- activity limited by pain in more progressive cases
- swelling is less likely due to the nature of tendinopathy
Diagnosis of Knee Tendonitis
We can diagnose most knee tendonitis with a thorough history and by pressing on the Patellar tendon.
An Ultrasound or MRI may also confirm knee tendonitis.
Cause of Knee Tendonitis
Patellar Tendonitis generally falls into the category of overuse injury. We often see it as a consequence of over-stressing the Patella tendon to the point of soreness.
The following external factors have links to knee tendonitis:
- Running, jumping, and landing-related activities
- Increase in training load, frequency or intensity
- Hard playing surface
- Change in footwear
But here's the thing. By definition, tendon loading and use are normal.
The body is designed to run and jump. It's designed to work hard. It's not fragile yet we fall into the trap of seeing these external factors as the cause rather than a trigger.
From what I see day-to-day it's potentially incorrect to label any tendonitis "overuse" for these reasons alone. Instead, it's more important to consider how you load your Patellar tendon, not just that you do at all.
Related: These three hidden factors set most knees up to fail.
Hidden Risk Factors
With every knee tendonitis, there are a number of pre-existing mechanical factors that change how we load the tendon. These set it up to fail when exposed to the external factors above.
These factors are hidden to the naked eye but can be found if you're willing to look for them.
Some of these are:
- Quadricep tightness
- Hamstring tightness
- Calf tightness
- Imbalances in muscle strength
- Weak gluteals
- Weak core
And although we are becoming more sophisticated at addressing these issues, I'm still seeing a few potential gaps in our thinking.
So let's discuss the influence of lower back dysfunction on the Patellar tendon.
What I'm Finding Clinically
Over the last few years, it seems that every knee tendonitis I've seen comes with stiffness in a very specific area of the lower back.
For the nerds out there, it often seems the most obvious around the T12-L3 segments.
For those unaware, this area incorporates the junction between the base of the ribcage and the top of the lumbar spine.

And what's interesting here is that we're not talking overt pain or discomfort, but specific stiffness. The kind you can only appreciate by directly poking and prodding.
Significantly, most patients have no awareness this area is stiff. Often because they have no back pain to alert them.
Why Is This Area Significant?
The super-nerds among us may recognize two things about the ~T12-L3 area.
Firstly, these segments house the Femoral nerve. This nerve supplies the Quadriceps and plots its course through the front of the thigh to the knee.
Secondly, these spinal segments also relate to the body's knee-related Dermatomes and Myotomes. Without going into too much detail these are sensory and motor connections leftover from our fetal development.
The point being there are direct and indirect connections between the lower back and the knee.
These connections may have functional and mechanical ramifications for the Patellar tendon if the associated spinal levels are stiff.
Clinically, this specific spinal stiffness seems to "pull slack" from associated nerves and soft tissue. This neural tension may act as a hand-brake to the knee forcing a long-term shift in the way we load the Patella tendon, potentially pre-empting the changes we see in knee tendonitis.
Where Is The Evidence?
At this stage, the only evidence I have to offer is clinical results.
I'm not aware of any robust research into this idea, but based on what I'm finding it hopefully won't be long until it exists.
Clinically, there seems a strong pattern of spinal stiffness with each patient diagnosed with Patellar tendonitis.
Furthermore, treating this spinal stiffness seems to consistently improve both pain and overall function.
From what I've come to understand, this spinal stiffness may be the underlying cause of knee tendonitis. It may pre-empt all of the training and exercise-related factors we associate with knee tendonitis. It may even precede other known factors like leg muscle imbalance and tightness.
Ultimately, spinal stiffness may add excessive resting tension to the patella tendon, setting it up for failure over time.
At this point it's important to acknowledge two things:
- I do not expect all lower back stiffness to cause knee tendonitis. Any predictive model generally fails in this context. However, I am yet to see a single patient over the last half a decade with knee tendonitis who doesn't have this specific spinal stiffness. Furthermore, it's rare to find someone whose knee symptoms don't benefit from treating this area of the spine.
- Despite such encouraging results I don't yet consider this a quick fix or magic bullet. The tendon clearly still has to remodel itself, but these results have given me a degree of confidence that treating the spine may hold the key to better prevention and treatment of knee tendonitis and a faster, more complete recovery.
Jaeger O'Meara
To highlight what I'm finding I'd like to discuss the complicated history of Australian Rules Football (AFL) player Jaeger O'Meara. Let's get to know him and what he's been through. It's worth noting Jaeger's knee was one of the most hotly discussed issues in the AFL for almost 4 years.
Jaeger's (Complicated) Injury History
As most Australians may already appreciate, Jaeger's a gun.
He was earmarked for greatness even before being drafted by the Gold Coast Suns back in 2011. He played two full seasons of AFL football (44 senior games) in his first two years in the system - a rare feat for a debutante. This included winning the 2013 Rising Star Award for the best young player in the game.
His rare mix of athletic gifts, football skills, and game sense had him touted as one of the best players of his generation.
Here are some highlights from his first year in the AFL as an 18-year-old.
Unfortunately, after such a bright start to his career things took a devastating turn.
On April 4th, 2015, Jaeger ruptured his right Patellar tendon during a preseason practice game in Cooparoo, Queensland when an opponent fell across his leg.
Interestingly, Jaeger required off-season surgery for severe bilateral knee tendonitis during the previous season. It was an issue that prevented him from training much, if at all that year. At the time, the Gold Coast Suns' medical staff were adamant the rupture and recent surgery were unrelated. It was deemed a freakish accident, despite the high likelihood of things being connected.
The following is a quick timeline of what followed his original Patellar tendon rupture in 2015:
- Surgery to repair Jaeger's ruptured Patellar tendon
- Expected to return to football in 12 months
- Returned to reserves football on limited game time in July 2016
- Succumbed to more knee soreness in just his 3rd reserves game back
- Ruled out for the rest of the 2016 season
- Poached by/reluctantly traded to Hawthorn at the end of 2016
- Hawthorn took a conservative approach to his rehabilitation
- Original aim to return to senior AFL football 4-5 rounds into the 2017 season
- Surpassed all expectations to play the first three games of the season including all three pre-season games
- Missed the next two for an unrelated knock to the same knee
- Returned in round 6, was limited and the sent away to work on his fitness and conditioning indefinitely.
- Returned sixteen weeks later to play the final 2 games of the season.
- Managed to play 21/24 games in 2018
- Played a further 21/22 games in 2019
And while following Jaeger's struggles from afar (I'm a Hawthorn supporter) I began to see some similarities between his issues and my patients.
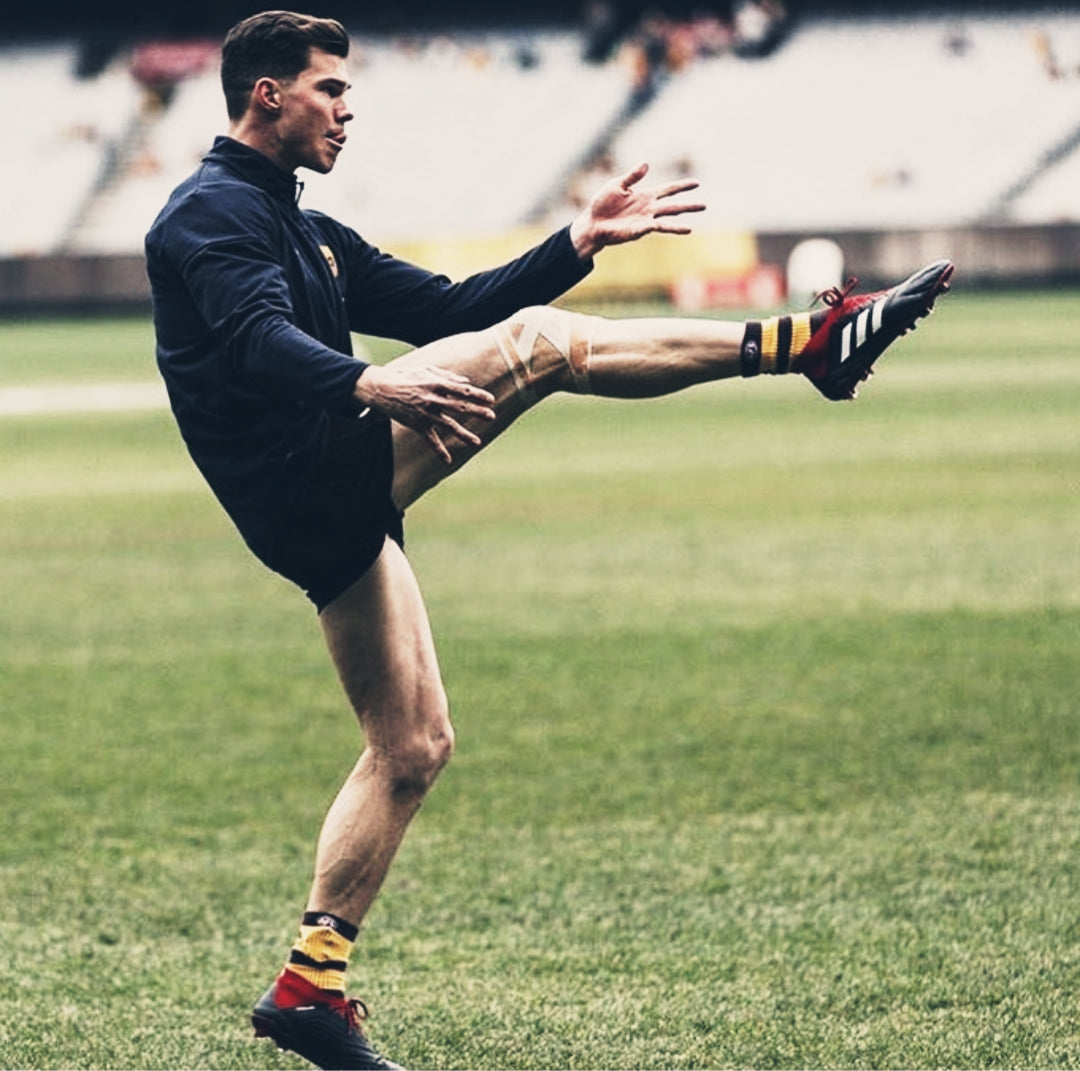
What's in a Picture?
I've found some images of Jaeger O'Meara (and the NFL's own Victor Cruz) to illustrate what I'm finding clinically.
It's always hard to infer anything from an image but they do frame what I'm seeing.

Can you see the very obvious spinal hinge in each of these images?
For those unaware, the spine is designed to bend. However, in a perfect world, this should be a global bend one, not a specific one. The reason for this is a global bend evenly distributes load across all spinal levels, whereas a direct hinge creates a hyper-focused area. This can force the spine to stiffen and tighten over time.
If these pictures truly reflect how Jaeger (and Victor) loads his spine when moving, then I'd expect the same to be true when he sits.
And with absolute respect to Jaeger, it's hard to find an image of him sitting in a good spinal position.

Here are two more I've pulled from his Instagram account.
His friend on the right isn't perfect either, but notice how much more flexed Jaeger is when he sits. The shadow obscures it a little but there's a distinct hinge in there.

Similarly, you can see how slouched Jaeger is in this image as well.
This is really important because in moments of high stimulus, the body defaults to what it knows.
And what it knows is often the direct consequence of these less-than-perfect positions and shapes. Not everyone's on holiday outside in the sunshine, but so many of us sit on the couch, sit at a desk, drive the car, etc. These moments often define the health and function of our spine for two simple reasons:
- We spend so much time doing them throughout the day
- It's rare we naturally do them in a good position
So with all this in mind, I'm finding that poor spinal shapes and postures seem to create a cascade of dysfunction that may better explain the onset, persistence, and re-occurrence of knee tendonitis.
If this is also the case with Jaeger O'Meara then it might help explain why he developed knee tendonitis when he did and lowered his threshold to rupturing his Patellar tendon.
It's worth noting that not every patient presents with as obvious a hinge as Jaeger (and Victor) but it speaks to the presence of poor spinal shapes and accrued stiffness nonetheless.
In my professional opinion, this information should shape the way we treat knee tendonitis. Not by changing the usual approach, but by allowing us to add greater depth to it.
The Best Treatment of Knee Tendonitis
Before we get to what I'd add to the treatment of knee tendonitis, it's important to cover what should already be commonplace.
Treatment of Patellar tendonitis should consist of the following things:
Manage Activity Levels
Knee tendonitis clearly has much to do with how you load your knee, but once painful it's still important to manage what you do with it as well.
Pure rest should be advised in extreme circumstances only. We need to use tendons (correctly) for remodelling, re-strengthening, and normalization to take place. Rest often makes sense for pain, however, it's more important to find a balance between doing too much and not enough. This will encourage the fastest recovery without constantly aggravating things.
Any increase in your symptoms - which do not settle in a reasonable amount of time, should be taken as doing "too much". The aim is always to be working comfortably below this threshold.
Pain Reduction
Pain is almost always the main concern for many patients - and rightfully so. However, it's important to understand that pain has a purpose. It gives us boundaries.
Use pain medication when things feel too painful or it heavily interrupts your quality of life, daily function or sleep. It should not be our default way of managing knee tendonitis.
The same goes for icing knee tendonitis.
Ice is useful for pain relief however it may come at a cost to the speed of your recovery. Here's an in-depth look at why we need to re-consider using ice to treat injury. Let me know what you think in the comments below.
As mentioned earlier, knee tendonitis does not usually involve inflammation but all tissue requires blood flow for optimal function. Ice negatively affects this.
Instead, work hard on improving why the Patellar tendon has become sore in the first place.
Improve How You Load the Patellar Tendon
At the end of the day, we need to normalize the way you load the Patella - not just rest and numb it with medication and ice.
The following are important to improve:
- Flexibility of Quadriceps
- The flexibility of Hamstrings, Calves, Gluteals
- Strength of Quadriceps (often eccentrically)
- The strength of Hamstrings, Calves, Gluteals
Massage, dry needling, and basic stretching are solid choices to improve the flexibility of these muscles.
Related: Consider using a power band to improve your flexibility.
Taping and Bracing
It can take a while to change the way we load the Patellar tendon meaning pain and discomfort can be slow to shift.
Patellar tendon taping can be a helpful way to maintain some level of function while your tissues take time to mobilize and strengthen.

By taping across the tendon with some rigid sports tape we can help disperse the load going through it.
Similarly, a Patellar tendon brace or strap can do the same.
Having said that, it's always important to think of taping and a brace for knee tendonitis as short-term options only. At some stage, your rehab exercises should make the brace or tape redundant.
How to Improve Spinal Function
I've left this until last to help emphasize my original point.
Relative rest, appropriate pain relief, taping, bracing, leg stretches and strength exercises serve a purpose when treating knee tendonitis.
But each may not address its potential root cause.
From what I'm finding clinically, we need to address poor spinal function as well.
And we can usually do this by focusing on three simple things:
- Reduce Spinal Stiffness:
Have your Physical Therapist mobilize above and below the base of your ribcage. Alternatively, take a lacrosse ball or foam roller and gently do it yourself. We seriously underrate this as an exercise for knee tendonitis

- Improve Trunk Strength:
Work with your Physical Therapist to find the most appropriate trunk/core strength exercises for your situation. In the meantime give the basic plank a try. It's simple, but a hugely effective way to begin re-strengthening your trunk and a neglected exercise for knee tendonitis.

- Practice Better Spinal Posture:
Mobility and strength will help improve the function of your spine, but it counts for little over time if you cannot re-train better spinal shapes.
As mentioned earlier, there seems a strong connection between spinal stiffness (and weakness) and poor spinal shapes throughout the day. It's almost impossible to expect your back to stay loose and strong over time if you can't maintain a more neutral spinal shape when it counts.

Conclusion
We do a great job managing knee tendonitis. However, I don't think we pay enough attention to spinal dysfunction and its impact on the onset, persistence, and risk of re-occurrence of knee tendonitis.
Conventional rehab is clearly still the foundation of recovery, but we might be able to better conquer a typically tricky condition by treating the mid-low back as well.
So with all of this in mind, I hope to arm those suffering from knee tendonitis (tendinopathy) with the same perspective I have come to learn.
If struggling, please don't just take my word for it. Speak to your Physical Therapist and get some feedback on your spine. In the meantime, prioritize straighter spinal shapes and go after any potential back stiffness yourself.